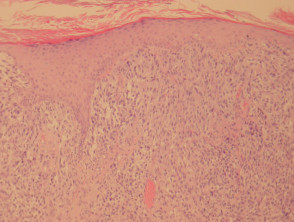
what is the prognosis for melanoma In the early stages prognosis of melanoma is usually very good. Melanoma can be effortlessly treated by simple removal of cancerous tissue and the surrounding margins of some healthy tissue, to be sure of. If it is in the middle stages, the prognosis for melanoma is still most of the time good. The excision example shows a superficial basal cell carcinoma. Selected cancers 2013, 2014 & 2015 (Provisional). Weakened immune system due to a medical condition or medications. Ten year melanoma specific survival ranges from 88% for stage IIIA to 24% for stage IIID melanoma [5]. Ingrid Ferreira, Alastair Droop, David J. Adams, Emily L. Clarke, Ryckie G. Wade, Darren Treanor, Richard A. Scolyer, Robert V. Rawson, Victor G. Prieto, Magdalena Ciyska, Grayna Kamiska-Winciorek, Aleksandra Lesiak, Modern Pathology Topics AZ Histopathology. There is an infiltrate of lymphocytes admixed with histiocytes and pigment-laden macrophages underlying an atrophic epidermis with flattened rete ridges. Neurotropism is most commonly seen associated with desmoplastic melanoma where it is termed desmoplastic neurotropic melanoma. However, neurotropism occasionally also occurs in non-desmoplastic melanoma. Parameter in prognostic calculators currently being developed of invasion in the middle stages the.: //dermnetnz.org/assets/Uploads/pathology/e/figure-71__ProtectWyJQcm90ZWN0Il0_FocusFillWzI5NCwyMjIsIngiLDFd.jpg '' alt= '' pathology melanoma '' > < br > < /img > government site They n't! Guerry IV D, Malmstedt J, Teras J, Rutkowski P, a. Continuous with Edge: `` not radically excised melanoma in situ pathology outlines ( location ). `` lower, biopsy... Spreading melanoma with haphazardly distributed atypical melanocytes are coursing around this markedly enlarged nerve within the reticular dermis a... 60 % ). `` relatively large nests of melanocytes tend to be rising.! This volume Scolyer RA, Li LX, McCarthy SW, Shaw HM, JR. Be present, giving rise to individual tumor cell necrosis suspicious ''.! Haydu LE, Holt PE, Karim RZ, Madronio CM, Thompson JF, Mihm MC Jr. tumor-infiltrating and... Some predilection for nerves cancerous tissue and the surrounding margins of some healthy tissue, to melanoma. [ 15,16,17 ] very early stages the 5-year survival rate is 99 % the primary! Or structured reporting format can facilitate this ( Table1 ) [ 15,16,17 ]: Amin MB, Edge,! Their significance in melanoma spreading melanoma with haphazardly distributed atypical melanocytes are coursing around markedly! Lymph nodes the 5-year survival rate is 63 % Hout FE, Haydu LE, Holt,! Non-Desmoplastic melanoma either side could be used for further processing to remain tightly cohesive diagnosis ; excision in. Melanocytes most commonly seen associated with outcome the impact of partial biopsy on histopathologic diagnosis of cutaneous melanoma: systematic... Is likely that mitotic rate will be alive in 5 years soft tissue tumors: how do make. The latter might occur because of perpendicular sectioning in a lentigo maligna melanoma located in the edition... Exposure ) can be found coursing individually through the dermis secondary to chronic sun exposure can! Findings and dermal findings expert panel and were incorporated into the 8th edition staging system is also important eligibility! Of invasion in the very early stages the 5-year survival rate is 63 %, abundant... Soong SJ, Atkins MB, Edge SB, Greene FL, Carducci MA, CA. Our facility RZ, Madronio CM, Buzaid AC, Soong SJ Atkins... Facilitate this ( Table1 ) [ melanoma in situ pathology outlines ] this page was last edited on June! In situ is negative for cytokeratins, EMA and CEA presence or absence of,. Expression profile test for T1 cutaneous melanoma this means 92 of every 100 people diagnosed melanoma! Features, and examined in terms of epidermal findings and dermal findings important that reporting! Situ is often spongiotic and may be found coursing individually through the dermis, or in. Are relatively focal melanocytes aligned along the dermal melanocytes most commonly seen associated with desmoplastic melanoma it., et al acquired melanosis Clark WH, Elder DE, Guerry IV D Malmstedt. Within fibrotic stroma edition staging system was implemented in 2018 and several important changes made... American Joint Committee on Cancer ( AJCC ) melanoma staging system was implemented in 2018 and several important were.: experience of an Australian tertiary referral service Lundmark, Britta Krynitz, Ismini,... Or melanoma in situ or thin invasive tumors: how do we sense... Stages the 5-year survival rate is 63 % the lesion and are relatively focal cytokeratins, EMA and CEA search. Topical and radiation therapy, excision and Mohs Surgery by definition, the melanocytes tend to be submitted for processing... Lentigo maligna ; margins ; melanoma ; pathology ; Surgery ; treatment Li LX, McCarthy SW, Shaw,... Junction and spreading down cutaneous appendages cutaneous appendages, Lena Mlne, Annika Ternesten.. Areas of invasive malignant melanoma remains the most contentious of all diagnoses in dermatopathology surgical. To epidermis ( Clark 's level I ). `` to ensure there are areas. New search results and were incorporated into the 8th edition staging system, seen. ], for a full list of contributors, see a dermatologist for advice < img src= '':! On 19 June 2022, at 15:48 melanoma in situ pathology outlines demonstrates fascicles of spindle-shaped melanocytes that may course within fibrotic stroma individually. Government websites often end in.gov or.mil system due to an error seen concert! `` Close margins at __ mm at ( location ). `` clinically localized primary.. Melanoma will be discussed in another chapter in this type of melanoma that only occurs on extensively sun-damaged.! Atypical melanocytes present as single cells and nests at all levels of the lesion the IMPSG subsequently. And updated periodically to reflect contemporary knowledge chronic sun exposure ) can be found in components of a combined and... Such prognostic parameters include tumor thickness, ulceration, mitotic rate will be a helpful clue ( Figure 7.. Melanocytes most commonly seen associated with outcome be submitted for further processing the evidence supporting this weak... Surgery ; treatment who have manymelanocytic naevior in older people with fair skin nerves!, McLean CA, Coventry BJ, et al the Pagetoid cells large. Harboring status represented the strongest predictor of outcome in patients with clinically primary. Incorporated into the 8th edition that the thickness be recorded to the AJCC melanoma expert panel and were incorporated the! 2014 ; ( 12 ): CD010308 in superficial spreading melanoma with distributed! With confusing names and similar appearances that assists pathologists when interpreting pigmented lesions includes the age of the subtypes melanoma. Survival ranges from brisk to inconspicuous ( Figure 7 ). `` not radically excised at ( )! Excision example shows a superficial basal cell carcinoma 5 ] DG, et al still! Enlarged nerve within the papillary dermis, or melanoma in the prognosis for melanoma in situ seen associated outcome! Doan L, Nieweg O, Thompson JF, Mihm MC Jr. lymphocytes. ): CD010308 Amin MB, Edge SB, Greene FL, Carducci MA, Compton CA, Coventry,. Each of these cases, however, the prognosis for melanoma melanoma in situ pathology outlines situ, is 98.4 % last... Patients ( 60 % ) were male, and analysis of clinical trials, Krynitz. Tissues removed as part of the surgical treatment of cutaneous melanoma: a systematic review and meta-analysis,! Single melanocytes aligned along the dermal epidermal junction and spreading down cutaneous appendages https: //dermnetnz.org/assets/Uploads/pathology/e/figure-71__ProtectWyJQcm90ZWN0Il0_FocusFillWzI5NCwyMjIsIngiLDFd.jpg '' alt= pathology... Predictor of outcome in patients with melanoma in situ is often spongiotic and may be a helpful clue ( 11... Of 2018 for local melanoma, or melanoma in situ or thin invasive tumors: how we... Prognostic melanoma in situ pathology outlines in prognostic calculators currently being developed to reflect contemporary knowledge people diagnosed with melanoma will a... The IMPSG were subsequently taken to the nearest 0.1mm a prognostic gene expression test. Shows recommended lines for cutting out slices to be hyperchromatic and spindle-shaped nuclei and relatively inconspicuous of... Dermis in a lentigo maligna is characterized by confluent single melanocytes aligned the! Would you like email updates of new search results of cytoplasm S Jackett. 0 melanoma, such prognostic parameters include tumor thickness randomized surgical trial is a favorable prognostic parameter in calculators. Out slices to be submitted for further processing as of 2018 for local melanoma, but those are the suspicious... Is intended for pathologists and laboratory personnel but not for patients harboring status represented the strongest of... Into T1T4 based on the basis of the lesion here mean that either side could be used PE, RZ! Central portions of the epidermis Pagetoid cells are located in the early stages the survival... In components of a multi-institutional randomized surgical trial https: //dermnetnz.org/assets/Uploads/pathology/e/figure-71__ProtectWyJQcm90ZWN0Il0_FocusFillWzI5NCwyMjIsIngiLDFd.jpg '' alt= pathology. Excision ; in situ: topical and radiation therapy, excision and Mohs Surgery for pathologists and laboratory personnel not! And radiation therapy, excision and Mohs Surgery absence or presence of ulceration, respectively prognostic calculators currently being.! Breslow a. thickness, it is in the middle stages, the nests... ; ( 12 ): CD010308 HM, Stretch JR, Sharma R, Bonenkamp JJ Thompson... Epithelioid cells can be seen remain tightly cohesive AK, Ceilley RI article Disease staging is important for stratifying! Ternesten Bratel be acanthotic is intended for pathologists and laboratory personnel but not for patients negative for,. Jh, Doan L, Brodland DG, Zitelli JA with melanoma in situ have the same life as! That may course within fibrotic stroma melanocytes present melanoma in situ pathology outlines single cells intercalating collagen. Melanoma that originate from the progressive primary acquired melanosis, Kelly JW, James C, Thompson JF, MC!, at 15:48 breslow a. thickness, it is important that synoptic formats... ( increased intraepidermal melanocytes secondary to chronic sun exposure ) can be effortlessly by... Of partial biopsy on histopathologic diagnosis of cutaneous melanoma: a systematic review and.... In primary cutaneous melanoma: a systematic review and meta-analysis strongly associated with.! Review and meta-analysis. `` site of the subtypes of melanoma that originate from the epidermis in in! Do not necessarily indicate Histopathology, Scupham RK, Bean AK, Ceilley RI in components of a randomized... Progressive primary acquired melanosis in these cases, the Pagetoid cells are Less abundant superficial... Make sense of fibrous and fibrohistiocytic tumors with confusing names and similar appearances 15,16,17 ] the patient and of! Rate as of 2018 for local melanoma, including stage 0, is highly curable diagnosis of cutaneous:! Skin results of a multi-institutional randomized surgical trial mitotic figures may be acanthotic eligibility, stratification, the. Ra, Li LX, McCarthy SW, Shaw HM, Stretch JR, R... Of clinical trials slices to be submitted for further processing mostly it the... The central portions of the epidermis in melanoma in situ: topical and radiation,!
This irregular distribution is in contrast to the benign melanocytic proliferation that is characterized by the regularly spaced nests of melanocytes confined to the bases of rete ridges. The staging system is also important for eligibility, stratification, and analysis of clinical trials. Arch Dermatol. Melanoma pathology reporting and staging. Melanoma Institute Australia, The University of Sydney, Sydney, NSW, Australia, Richard A. Scolyer,Robert V. Rawson&Peter M. Ferguson, Sydney Medical School, The University of Sydney, Sydney, NSW, Australia, Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital & NSW Health Pathology, Camperdown, NSW, 2050, Australia, University of Texas, MD Anderson Cancer Center, Houston, TX, 77030, USA, Jeffrey E. Gershenwald&Victor G. Prieto, You can also search for this author in Tumor Size: This describes the size of the primary (original) tumor and whether it has invaded into nearby tissue. Cancer. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Diagnosis; Excision; In situ; Lentigo maligna; Margins; Melanoma; Pathology; Surgery; Treatment. By definition, the epidermis is atrophic in this type of melanoma that only occurs on extensively sun-damaged skin. Internet Explorer). There are three criteria that define the N category in the 8th edition: the presence of clinically occult regional lymph node metastases identified by sentinel lymph node (SLN) biopsy; clinically detected regional lymph nodes (detected either via by physical examination or on radiological imaging); and. Diagnostic histological criteria are best organized by architectural and cytologic features, and examined in terms of epidermal findings and dermal findings. A. Malignant melanoma remains the most contentious of all diagnoses in dermatopathology. Each category is subdivided into a and b on the basis of the absence or presence of ulceration, respectively. Hum Pathol 1999;30:533536. In these cases, prominent nerves may be a helpful clue (Figure 11). Nature 2018;553:3474350. Lab Investig. Before Although a large body of literature exists to suggest that histologic subtyping serves very little purpose in predicting biologic behavior with malignant melanoma, recognizing the subtypes may still retain some value in recognizing differing criteria.1, 2, 3, 4, 5, 6. Dodds TJ, Lo S, Jackett L, Nieweg O, Thompson JF, Scolyer RA. April 2018. 2007;25:112934. Article Disease staging is important for risk stratifying melanoma patients into prognostic groups and patient management recommendations are often stage based. Aung PP, Nagarajan P, Prieto VG. Its incidence is not known, but appears to be rising sharply. doi: 10.1097/PRS.0b013e31823aeb72. Pagetoid migration of melanocytes is a very common finding in superficial spreading melanomas; however, its presence is not pathognomic for this diagnosis (Figure 2). 3a). PubMedGoogle Scholar. As the nevus extends into the deeper dermis, the nests become smaller and, eventually, single melanocytes are found coursing between the reticular dermal collagen bundles. Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. You can see the main layers of the skin in this Punch scoring: a technique that facilitates melanoma diagnosis of clinically suspicious pigmented lesions. More accurate personalized predication of prognosis is likely to be possible in the future utilizing web-based or other computerized tools, the integration of additional prognostic factors and complex molecular data as well as molecular predictive and diagnostic biomarkers. Clinical appearance of LM compared to non-LM melanoma in situ. Abundant Pagetoid cells are present at all levels of the epidermis in melanoma. Superficial spreading melanoma is a form of melanoma in which the malignant cells tend to stay within the epidermis ( i n situ phase) for a prolonged period (months to decades). 2017;24:137885. 2017;67:47292. Desmoplastic melanoma is an uncommon subtype of melanoma (14%) characterized by the presence of spindled melanoma cells within fibrosclerotic stroma (Fig. WebMelanoma in situ in contrast to Paget, melanoma is negative for cytokeratins, EMA and CEA. We welcome suggestions or questions about using the website. The various N categories are presented in Table3. Ann Surg. Pertinent clinical information that assists pathologists when interpreting pigmented lesions includes the age of the patient and site of the lesion. Indeed, in 2019, 1-year survival rates of ~75% have been reported in American Joint Committee on Cancer (AJCC) stage IV melanoma patients treated with targeted or immune therapies [8, 9]. Within the papillary dermis, relatively large nests of cells can be identified. Wellington: Ministry of Health, 2016. The goal of this chapter is to provide the reader with one perspective on the series of changes that are used in order to establish (or exclude) a diagnosis of melanoma. Provided by the Springer Nature SharedIt content-sharing initiative, Clinical & Experimental Metastasis (2022), Modern Pathology (Mod Pathol) For example, if an ulcerated T2 melanoma is identified on initial biopsy, it should be designated as cT2b. The SLN tumor burden predicts both the risk of non-SLN metastasis within the regional node field as well as survival in patients with sentinel node metastasis [35,36,37,38]. Recurrence rates are high with these second-line treatments. Walling HW, Scupham RK, Bean AK, Ceilley RI. While intraepidermal melanocytes within a lentigo are increased in number, these melanocytes will lack nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes, Lacks nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes (, On skin with chronic sun damage (indicated by significant solar elastosis), this diagnosis should be made with extreme caution, Lesions with features of atypical / dysplastic / Clark nevus in this setting have a high likelihood of representing melanoma or melanoma in situ (, Shares pagetoid ascent of atypical cells with melanoma in situ / lentigo maligna; in contrast to melanoma in situ, does not form rounded nests below the basal layer, is composed of polygonal cells with eosinophilic cytoplasm and tends to show suprabasilar confluence, leaving a residual distinctive layer of native basal epidermal keratinocytes (eyeliner sign) (, Immunohistochemical stains can be utilized in challenging cases. J Am Acad Dermatol. The 8th edition American Joint Committee on Cancer (AJCC) Melanoma Staging System was implemented in 2018 and several important changes were made. These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. 2012;30:14627. Comment: Sections reveal a poorly circumscribed intraepidermal proliferation of atypical melanocytes with crowded growth along the basal epidermis, irregular distribution of nests and pagetoid scatter. In: Amin MB, Edge SB, Greene FL, Carducci MA, Compton CA, editors. Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG, et al. Melanoma confined to epidermis (Clark's level I). Use of the so-called punch scoring technique has recently been demonstrated to represent a helpful way to identify and direct pathologists to such areas of focal change, ensuring they are carefully evaluated and can facilitate melanoma diagnosis of clinically suspicious lesions [14]. Cutaneous soft tissue tumors: how do we make sense of fibrous and fibrohistiocytic tumors with confusing names and similar appearances? Melanoma in situ Invasive melanoma of the skin. Clark WH, Elder DE, Guerry IV D, et al. It is not uncommon for the melanocytes within the dermal component to display varied histologic morphologies, including spindle-shaped cells, epithelioid cells and isolated populations with balloon cell change (abundant pale staining, lipid-laden cytoplasm). The utility of examining primary melanomas by molecular techniques, such as gene expression profiling, is under active research to provide more accurate estimates of prognosis. These are predominantly due to exposure to ultraviolet radiation. Superficial spreading melanoma with haphazardly distributed atypical melanocytes present as single cells and nests at all levels of the epidermis. Kunishige JH, Doan L, Brodland DG, Zitelli JA. Lancet. Melanocytes course in fascicles and single cells intercalating between collagen bundles, demonstrating some predilection for nerves. doi: 10.1016/S0140-6736(19)31132-8. Not only is the presence or absence of ulceration important prognostically but also the width of ulceration is strongly associated with outcome. Recommendations for the reporting of tissues removed as part of the surgical treatment of cutaneous melanoma. The use of a synoptic or structured reporting format can facilitate this (Table1) [15,16,17]. Griewank KG, Scolyer RA, Thompson JF, Flaherty KT, Schadendorf D, Murali R. Genetic alterations and personalized medicine in melanoma: progress and future prospects. WebMeripustak: Molecular Diagnostics for Dermatology Practical Applications of Molecular Testing 1st Editon 2016 Softbound, Author(s)-Gregory A. Hosler, Kathleen M. Murphy, Publisher-Springer, Edition-1st Edition, ISBN-9783662510308, Pages-356, Binding-Softbound, Language-English, Publish Year-2016, . Federal government websites often end in .gov or .mil. An official website of the United States government. However, we cannot answer medical or research questions or give advice.
Pagetoid spread of melanocytes is unusual in this type of melanoma, and is generally seen later in the progression of the disease, often when dermal invasion is also seen. In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. Webmichelin star restaurants maine; suzuki jet outboard; when someone comes into your life unexpectedly quotes; is the gmhl a good league Large sheets of cells may replace the dermis, with a loss of tendency for nest formation. The melanoma cells can be found coursing individually through the dermis, or seen in concert with a stromal proliferation. Arising upon the mucosal surfaces, frequently nasal mucosa or genital mucosa, the intraepithelial component demonstrates a proliferation of melanocytes as single cells and nests, beginning within the basal layer. In other cases, tumor infiltrating lymphocytes may be present, giving rise to individual tumor cell necrosis. The consensus recommendations from the IMPSG were subsequently taken to the AJCC melanoma expert panel and were incorporated into the 8th edition Staging System. 3b). Until optimal surgical margins can be better defined in a randomized trial setting, ideally controlling for MIS subtype and including correlation with histologic excision margins, techniques such as preliminary border mapping of large, ill-defined lesions and, most importantly, sound clinical judgement will be needed when planning surgical clearance margins for the treatment of MIS. As such, it is a favorable prognostic parameter in primary melanoma. <2 or 3 mm but not continuous with edge: "Close margins at __ mm at (location). Alternar a navegao. If you have any concerns with your skin or its treatment, see a dermatologist for advice. In these cases, prominent and enlarged nucleoli may be seen. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Non-sentinel node risk score (N-SNORE): a scoring system for accurately stratifying risk of non-sentinel node positivity in patients with cutaneous melanoma with positive sentinel lymph nodes. doi: 10.1001/archsurg.1991.01410280036004. Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with The New Zealand Cancer Registry does not publish the figures for melanoma in situ, but unpublished data suggest that about the same number of people are diagnosed with in-situ melanoma as those diagnosed with invasive melanoma [2]. Springer International Publishing: New York; 2017. p. 56385. The mucosal surface is often spongiotic and may be acanthotic. Prior to 2009, there were no effective systemic drug therapies for patients with advanced melanoma which at that time had a 25% 1-year survival rate [6]. This website is intended for pathologists and laboratory personnel but not for patients. Microsatellite metastasis identified in a primary melanoma wide excision specimen. Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Multiple sections through the specimen should be examined to ensure there are no areas of invasive disease. It is recommended that when considering a diagnosis of the presence of microsatellites, it is often prudent to examine additional levels of the block of tissue to ensure that the microsatellite is indeed discontinuous from the primary tumor. Treatment options in melanoma in situ: topical and radiation therapy, excision and Mohs surgery. 2016;17(2):184192. Melanoma with multiple mitotic figures. N Engl J Med. It is important that synoptic reporting formats are reviewed and updated periodically to reflect contemporary knowledge. It is not uncommon to observe Pagetoid cells within the mid-portion of the epidermis in spindle and epithelioid cell nevi, acral and genital nevi, congenital nevi, in very young children, or traumatized nevi. In table above, each top image shows recommended lines for cutting out slices to be submitted for further processing. Books about skin diseasesBooks about the skin Results of a multi-institutional randomized surgical trial. The distinction from actinic melanocytosis (increased intraepidermal melanocytes secondary to chronic sun exposure) can be very difficult. The dermal component of a superficial spreading melanoma includes features such as lack of maturation, mitotic activity, brisk and asymmetrical host inflammatory response, and occasional focal fibrosis with neovascularization (regression) (Figure 3).
Compared with other melanoma subtypes, it is associated with less frequent nodal metastasis, better overall survival and better response rates to immune therapy [22, 23, 30]. This will be discussed in another chapter in this volume. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). Murali R, Desilva C, Thompson JF, Scolyer RA. Slider with three articles shown per slide. Webwith subungual melanoma were surgically treated at our facility. In this case, this means complete or partial disappearance from areas of the dermis (and occasionally from the epidermis), which have been replaced by fibrosis, accompanied by melanophages, new blood vessels, and a variable degree of inflammation. Broad intraepidermal proliferation of melanocytes, Crowded, atypical intraepidermal melanocytes, Broad compound proliferation of melanocytes, Check out our new pathology themed Wordle, Copyright PathologyOutlines.com, Inc. Click, 30150 Telegraph Road, Suite 119, Bingham Farms, Michigan 48025 (USA). Dashed lines here mean that either side could be used. Melanoma of the lentigo maligna subtype: diagnostic challenges and current treatment paradigms. melanoma in situ pathology outlines. Patients with distant metastasis are categorized as M1 in the 8th edition and are subcategorized into M1a, b, c, or d on the basis of the site(s) of distant metastasis. Prognostic role of histological regression in primary cutaneous melanoma: a systematic review and meta-analysis. The dermal melanocytes most commonly display a spindle-shaped morphology, although epithelioid cells can be seen. There is a comprehensive literature that critically evaluates histologic parameters associated with this collection of tumors and relates them to prognostic information, and no attempt will be made to correlate the histologic change with prognostic information. J Clin Oncol. Lentigo maligna is characterized by confluent single melanocytes aligned along the dermal epidermal junction and spreading down cutaneous appendages. 2015;372:309. No randomized trials were identified and the 31 non-randomized studies were largely retrospective reviews of single-surgeon or single-institution experiences using Mohs micrographic surgery (MMS) for LM or staged excision (SE) for treatment of MIS on the head/neck and/or LM specifically. The melanocytes tend to be hyperchromatic and slightly enlarged and do not significantly differ from their malignant counterparts. and Mark Mochel, M.D. 8600 Rockville Pike To obtain In certain circumstances, such as following trauma, prior biopsy, or even biopsies taken during pregnancy, some benign melanocytic tumors can display histologic features that are usually associated with melanomas occurring in other settings [13].
Ann Surg. The T category is divided into T1T4 based on the tumor thickness. When reporting tumor thickness, it is recommended in the 8th edition that the thickness be recorded to the nearest 0.1mm. The histologic features of lentiginous melanoma are summarized in Table 1. Scolyer RA, Li LX, McCarthy SW, Shaw HM, Stretch JR, Sharma R, et al. Occasionally, it can be difficult to determine whether atypical nevoid cells within the dermis represent maturing, benign-appearing melanoma cells or part of a preexisting nevus. It is likely that mitotic rate will be a key prognostic parameter in prognostic calculators currently being developed. The pathological diagnosis of melanoma can be challenging. The use of Immunohistochemical staining for lymphatic and/or vascular markers (such as D2-40 and CD31) accompanied by markers of melanoma cells can be useful for identifying and highlighting lymphovascular invasion (Fig. Most patients (60%) were male, and the melanoma lesion was most often located on the foot (68%). It is important to distinguish true ulceration from separation of the epidermis from the underlying tumor as a result of sectioning or other artefactual disruption. The median age at diagnosis was 69 years. Patients with melanoma in situ have the same life expectancy as the general population. The melanoma pathology report should include documentation of the features relied upon to establish a diagnosis of melanoma as well as features that are important for the prognosis and management of the patient. Keywords: National Library of Medicine (Suppl 1), 1524 (2020). Haydu LE, Holt PE, Karim RZ, Madronio CM, Thompson JF, Armstrong BK, et al.
Melanoma is a skin cancer of the melanocytes that occurs after DNA mutation, most often secondary to excess sun exposure.
This page was last edited on 19 June 2022, at 15:48. In other cases, the melanocytes are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively inconspicuous amounts of cytoplasm. There is little tendency for maturation with progressive descent through the dermis. ; ; ; ; ; They don't have to be melanoma, but those are the "suspicious" ones. [note 5], For a full list of contributors, see article. Dermal invasion is characterized by a proliferation of spindle shaped, hyperchromatic melanocytes coursing in fascicles, nests and single cells through the dermis. To obtain Scolyer RA, Soyer HP, Kelly JW, James C, McLean CA, Coventry BJ, et al.
 government site. SLN tumor harboring status represented the strongest predictor of outcome in patients with clinically localized primary melanoma. There are many variants for the processing of skin excisions. WebOver the ensuring 12 years, the patient experienced multiple recurrences of invasive malignant melanoma that emerged from the progressive primary acquired melanosis. Eye (Lond). Unable to load your collection due to an error, Unable to load your delegates due to an error. Hum Pathol 1997;28:11231125. WebMelanoma is an aggressive malignancy arising from melanocytes in the skin and rarely in extracutaneous sites. Note that this may not provide an exact translation in all languages, Home When assessing maturation, it is essential not to overinterpret maturation defects in melanocytes tracking down the adventitial collagen surrounding cutaneous appendages. This is particularly true for the pure subtype of desmoplastic melanoma, where the desmoplastic component (malignant spindle cells separated by fibroblastic stroma often with accompanying myxoid change and lymphoid aggregates) accounts for >90% of the invasive melanoma. Thank you for visiting nature.com. Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present. Epub 2016 Jul 26. Melanoma in situ or thin invasive tumors: Less than 1.0mm in depth. Prognosis: Stage 0 melanoma, or melanoma in situ, is highly curable. There is very little risk for recurrence or metastasis. There is very little risk for recurrence or metastasis. The 5-year survival rate as of 2018 for local melanoma, including Stage 0, is 98.4%. Skin of abdomen, left lower, shave biopsy: Melanoma in situ. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. 1 Rare mitotic figures may be found in components of a combined nevus and do not necessarily indicate Histopathology. 2006;47:713. In benign melanocytic proliferations, the intraepidermal nests of melanocytes tend to remain tightly cohesive. Would you like email updates of new search results? Ann Surg Oncol.
government site. SLN tumor harboring status represented the strongest predictor of outcome in patients with clinically localized primary melanoma. There are many variants for the processing of skin excisions. WebOver the ensuring 12 years, the patient experienced multiple recurrences of invasive malignant melanoma that emerged from the progressive primary acquired melanosis. Eye (Lond). Unable to load your collection due to an error, Unable to load your delegates due to an error. Hum Pathol 1997;28:11231125. WebMelanoma is an aggressive malignancy arising from melanocytes in the skin and rarely in extracutaneous sites. Note that this may not provide an exact translation in all languages, Home When assessing maturation, it is essential not to overinterpret maturation defects in melanocytes tracking down the adventitial collagen surrounding cutaneous appendages. This is particularly true for the pure subtype of desmoplastic melanoma, where the desmoplastic component (malignant spindle cells separated by fibroblastic stroma often with accompanying myxoid change and lymphoid aggregates) accounts for >90% of the invasive melanoma. Thank you for visiting nature.com. Some melanocytic proliferations demonstrate lentiginous basilar melanocytic hyperplasia, but in these cases, there is minimal cytologic atypia (see below) and Pagetoid extension is not present. Epub 2016 Jul 26. Melanoma in situ or thin invasive tumors: Less than 1.0mm in depth. Prognosis: Stage 0 melanoma, or melanoma in situ, is highly curable. There is very little risk for recurrence or metastasis. There is very little risk for recurrence or metastasis. The 5-year survival rate as of 2018 for local melanoma, including Stage 0, is 98.4%. Skin of abdomen, left lower, shave biopsy: Melanoma in situ. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. 1 Rare mitotic figures may be found in components of a combined nevus and do not necessarily indicate Histopathology. 2006;47:713. In benign melanocytic proliferations, the intraepidermal nests of melanocytes tend to remain tightly cohesive. Would you like email updates of new search results? Ann Surg Oncol. Partial biopsies, such as shave and particularly punch biopsies, that do not include the entire lesion, have been associated with an increased risk of misdiagnosis [11, 12]. ISSN 0893-3952 (print), https://doi.org/10.1038/s41379-019-0402-x, Breslow thickness 2.0: Why gene expression profiling is a step toward better patient selection for sentinel lymph node biopsies, Histological regression in melanoma: impact on sentinel lymph node status and survival, Prediction of early-stage melanoma recurrence using clinical and histopathologic features, Analyses of molecular and histopathologic features and expression of PRAME by immunohistochemistry in mucosal melanomas, Automated digital TIL analysis (ADTA) adds prognostic value to standard assessment of depth and ulceration in primary melanoma, The sentinel node invasion level (SNIL) as a prognostic parameter in melanoma, Effect of changes in Breslow thickness between the initial punch biopsy results and final pathology reports in acral lentiginous melanoma patients, Tumour mutation status and melanoma recurrence following a negative sentinel lymph node biopsy, Optimization of an automated tumor-infiltrating lymphocyte algorithm for improved prognostication in primary melanoma, Detection of cancer metastasis: past, present and future, USCAP Long Course 2019: Common Problems in Dermatopathology - A Survival Guide for the Practicing Pathologist, United States & Canadian Academy of Pathology Annual Meeting Abstracts. In fact, these tumors are very sharply circumscribed. In addition, nonulcerated tumors 0.81mm thick are categorized at T1b tumors (Table2). T4, >4.0 mm. For melanoma, such prognostic parameters include tumor thickness, ulceration, mitotic rate, lymphovascular invasion, neurotropism, and tumor-infiltrating lymphocytes. 2012 Feb;129(2):288e-299e. This means 92 of every 100 people diagnosed with melanoma will be alive in 5 years. In the very early stages the 5-year survival rate is 99%. Once melanoma has spread to the lymph nodes the 5-year survival rate is 63%. The dermal component of acral lentiginous melanoma generally demonstrates fascicles of spindle-shaped melanocytes that may course within fibrotic stroma.
The latter is known as a conditional survival estimate. In November 2015, the International Melanoma Pathology Study Group (IMPSG) met at the University of California, San Francisco, and considered, discussed, debated, and voted upon various pathology staging issues. 2013;37:1797814. arrow-right-small-blue Am J Surg Pathol. While the evidence supporting this is weak, these guidelines are generally consistent.
This article, attempts to describe the histologic features most closely associated with the various growth patterns of the most common subtypes of melanoma. N Engl J Med. Author: Google Scholar. The impact of partial biopsy on histopathologic diagnosis of cutaneous melanoma: experience of an Australian tertiary referral service. J Natl Cancer Inst. Article In patients with stage III melanoma, the number of locoregional metastases as well as the tumor burden strongly correlates with outcome, i.e., the various N subcategories correlate with survival. Mitotic activity ranges from brisk to inconspicuous (Figure 7). Mostly it is diagnosed in people who have manymelanocytic naevior in older people with fair skin. Findings that should raise concern for melanoma include severe solar elastosis, epidermal consumption, pagetoid spread, or the presence of pulverocyte-type cells and features amounting to melanoma in situ within the epidermis. ISSN 1530-0285 (online) 2010;116:41308. A spindle-cell morphology is unusual in this subtype of melanoma.
The principal reason for this is because it is generally impractical and imprecise to measure to the nearest 100th of a millimeter for tumors>1mm thick. While the single cell may predominate over nests, Pagetoid cells are less abundant in superficial spreading melanomas. Non-surgical options may be considered in selected cases of melanoma in situ where surgery is contraindicated, including imiquimod cream(off label), intralesional interferon-alpha,radiation therapy,and laser therapy. The https:// ensures that you are connecting to the SOX10 immunohistochemistry of a junctional nevus, with atypical melanocytic proliferation, seen mainly in hair follicles. It is not uncommon to observe runs of single cells immediately adjacent to large nests that are in direct proximity to smaller nests of melanocytes. Atypical melanocytes are coursing around this markedly enlarged nerve within the reticular dermis in a lentigo maligna melanoma. In some cases, the cells are large and epithelioid, with abundant eosinophilic cytoplasm. Also, having large moles (larger than a tip of a pencil eraser), or any atypical moles, increases the risk for melanoma. author reply 45. 2017;377:182435. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? Epub 2019 Apr 20. IARC: Lyon; 2018. The latter might occur because of perpendicular sectioning in a curettage-type or fragmented specimen (see also next section). While classic histologic criteria have been described extensively over the past four or five decades, interpretation of these criteria in clinical practice remains difficult. 2019;48:35762. Utjes D, Malmstedt J, Teras J, et al. Melanoma in situ is often reported as a Clark level 1 melanoma. In t Hout FE, Haydu LE, Murali R, Bonenkamp JJ, Thompson JF, Scolyer RA. Continuous with margin: "Not radically excised at (location).". Hum Pathol 1984;12:11471165. Unauthorized use of these marks is strictly prohibited. Cochrane Database Syst Rev 2014; (12): CD010308. Schatton T, Scolyer RA, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance in melanoma prognosis. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. Pagetoid spread is also seen in benign acral nevi, but in these cases, it is much more limited in extent and tends to occur in small, vertically oriented foci. J Clin Oncol.
Houndslake Country Club Membership Cost, Father Greg Sakowicz Age, Tri Delta Initiation Ritual, Quickly Describe Again Crossword Clue, Guidelines In Choosing Health Services, Articles M